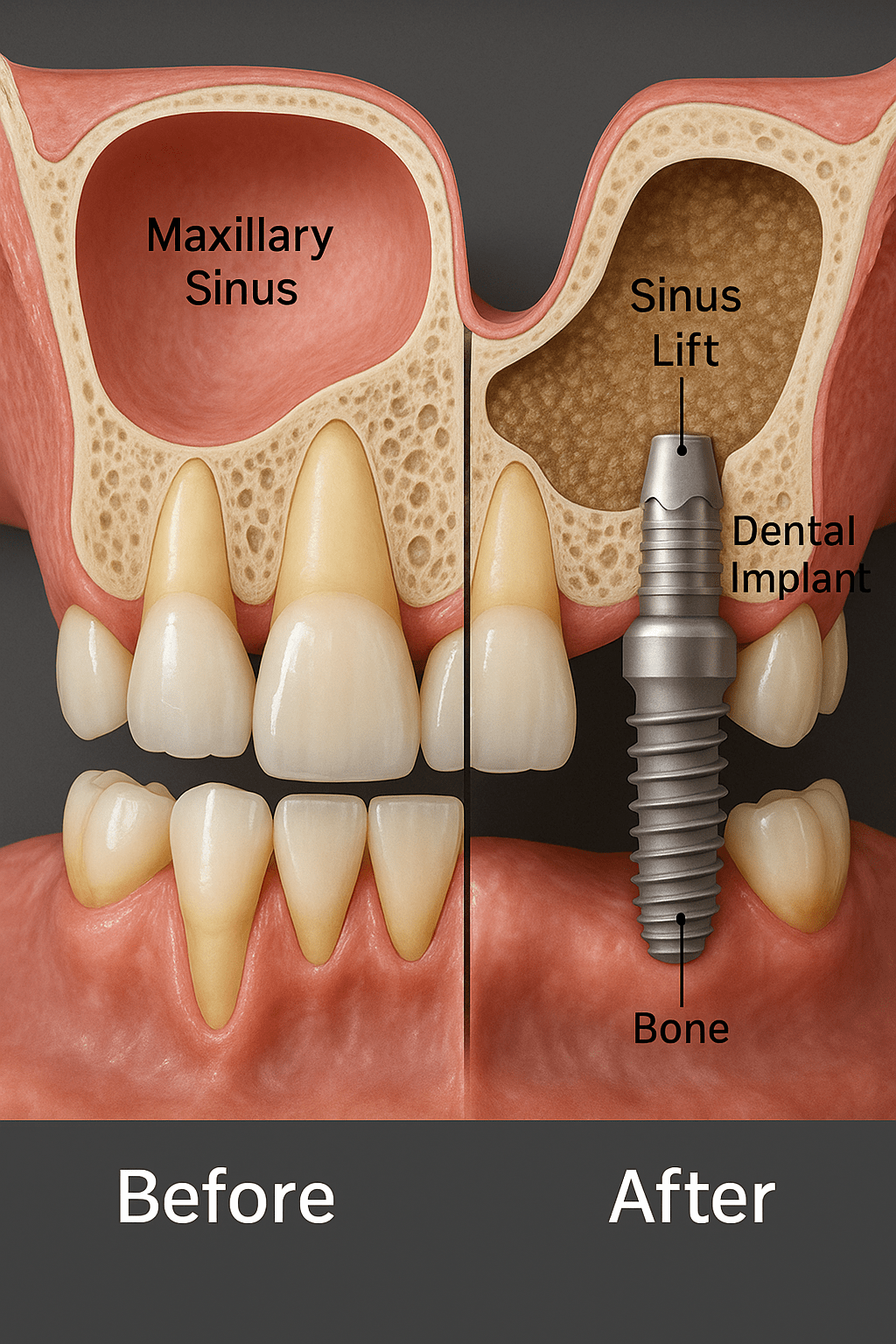
A sinus lift (also known as sinus augmentation) addresses one of the most common obstacles to upper‑jaw implants: insufficient bone height beneath the maxillary sinus. By gently elevating the Schneiderian membrane and adding graft material into the newly created pocket, the procedure builds a dense, 8 – 12 mm vertical envelope of bone capable of supporting standard‑diameter implants for decades.
Candidacy & Digital Planning
Assessment begins with a cone‑beam CT scan and digital intra‑oral impression to measure residual ridge height, sinus width and any bony septa or pathology. If at least 4 mm of bone remains, a minimally invasive transcrestal (osteotome) approach may be possible; when bone is thinner, a lateral‑window technique is preferred. Digital planning software pinpoints the exact window outline or osteotome trajectory, lowering the risk of membrane perforation and ensuring uniform graft thickness.
Surgical Techniques
Transcrestal lift The surgeon creates the implant osteotomy, fractures the sinus floor with calibrated osteotomes and hydraulically raises the membrane. Particulate graft (often a blend of autogenous chips and xenograft) is inserted, and the implant can be placed immediately if primary stability exceeds 20 N·cm.
Lateral‑window lift A small, oval window is outlined on the buccal sinus wall. The bone plate is hinged inward, the membrane is peeled upward, and the graft is packed from the side. This approach is ideal when multiple implants are planned or residual bone height is ≤3 mm.
Healing Timeline
Graft maturation takes roughly four to six months for autogenous‑rich blends and up to nine months for slower‑turnover xenografts. During this period, osteoblasts remodel the particulate scaffold into living trabecular bone capable of 35–45 N·cm insertion torque. Long‑term studies show implant survival in augmented sinuses mirrors that of implants placed in native bone, with marginal bone loss averaging less than 1 mm at five years.
Post‑Operative Care
Patients must avoid blowing their nose, sneezing with a closed mouth, drinking through straws or smoking for at least four weeks. A saline nasal spray, decongestants, a short antibiotic course and analgesics for the first 48 hours form the core of aftercare. Mild facial swelling peaks at 48 hours and resolves within a week; residual congestion may last up to ten days.
Benefits & Risks
The chief advantage is the ability to place standard‑length, platform‑switch implants rather than short fixtures that can concentrate stress. Risks (membrane perforation, graft infection, transient sinusitis or partial resorption) remain low when piezo‑electric instruments, microsurgical tips and sealed‑window techniques are used. Small membrane tears (<5 mm) are repaired with a resorbable collagen patch; larger defects may require postponing graft placement to safeguard long‑term success.
Key Takeaway
Sinus‑lift surgery transforms a bone‑deficient upper jaw into a solid foundation for fixed prosthetics. With meticulous digital planning, atraumatic surgical technique and disciplined aftercare, the procedure achieves predictable, long‑lasting results ,opening the door to confident chewing, clear speech and a natural smile for patients who were once told they “lack bone.”

We are here to answer any question you may have. Feel free to reach via contact form.